





 |
ICP811S - INTERGRATED CLINICAL PATHOPHYSIOLOGY - 1ST OPP - JUNE 2022 |
|
|
1 Page 1 |
▲back to top |
nAm I BI A un IVERSITY
OF SCIEnCE Ano TECHnOLOGY
Faculty of Health, Applied Sciences and Natural Resources
Department of Health Sciences
QUALIFICATION: BACHELOROF MEDICAL LABORATORYSCIENCES
QUALIFICATIONCODE: 08BMLS
LEVEL:8
COURSE: INTEGRATED CLINICAL PATHOPHYSIOLOGY COURSECODE: ICP8115
DATE: JUNE 2022
SESSION: THEORY
DURATION: 3 HOURS
MARKS: 170
FIRSTOPPORTUNITYEXAMINATION
EXAMINER(S) Ms Roselin Tsauses, Mrs Fredrika Engelbrecht, Dr Maurice Nyambuya, Dr
Munyaradzi Mukesi
MODERATOR: Prof Glenda Davison
INSTRUCTIONS
1. Answer ALL the questions.
2. Write clearly and neatly.
3. Number the answers clearly.
PERMISSIBLEMATERIALS
1. Pen
2. Calculator
THIS QUESTION PAPERCONSISTSOF 6 PAGES(Including this front page)
Page 1 of 6
|
|
2 Page 2 |
▲back to top |
SECTION A (79 MARKS)
Question 1
[10]
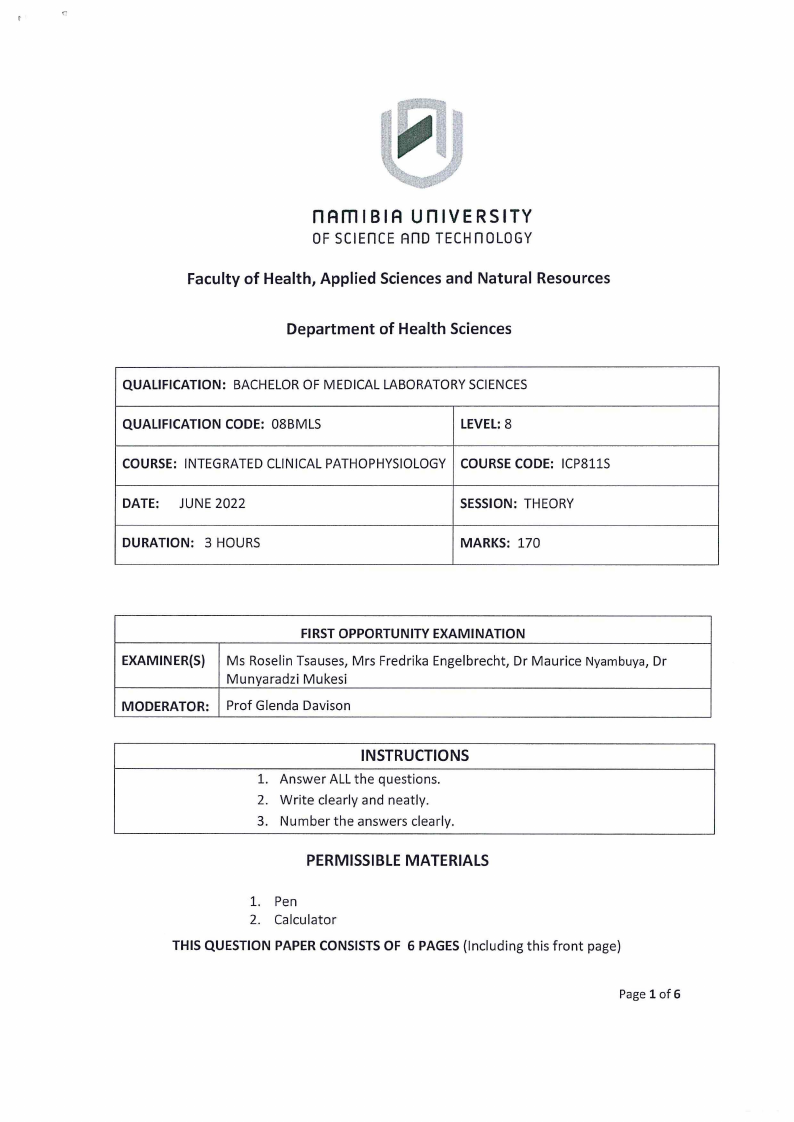
1.1 An 11-month-old girl with 1-month history of emesis, gagging, and choking with textured
foods was brought to her paediatrician by her parents and, after examination, was
admitted for management. The prior month, she was briefly admitted to the hospital for
a respiratory syncytial virus bronchiolitis and was given oral prednisone 10 mg twice a day
for 5 days. On current admission, the baby underwent an oesophagogastro-
duodenoscopy. The middle to distal oesophagus was covered with yellow-white plaques
scattered over the mucosa. The mucosa was hyperaemic and friable, and the plaques
could not be washed off. The lesions bled easily at the site of attachment, where they
were brushed for cytology. Biopsies were also taken. Fungal pseudo hyphae and spores,
morphologically consistent with Candida species, were also present as seen in the figure
below.
a) What are the clinical presentations of candidiasis in different groups of patients? (4)
b) Discuss non-cytological methods used to identify Candida spp. in the laboratory. (6)
Question 2
[14]
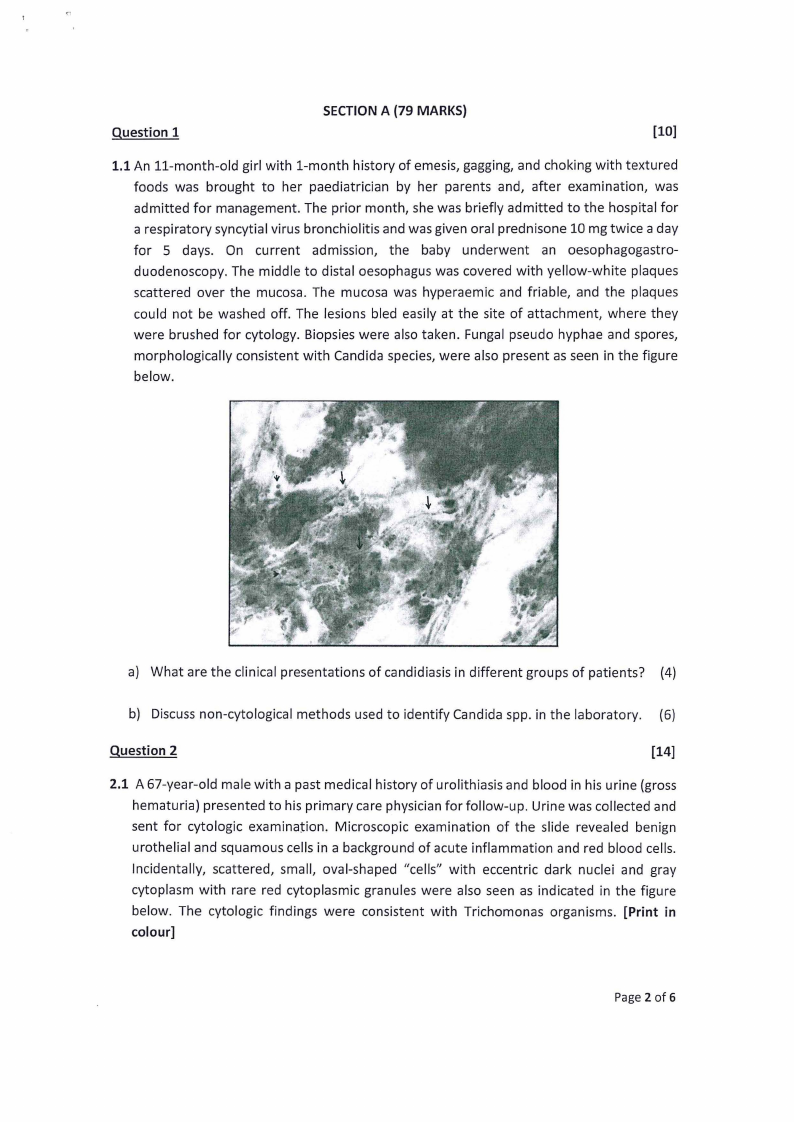
2.1 A 67-year-old male with a past medical history of urolithiasis and blood in his urine (gross
hematuria) presented to his primary care physician for follow-up. Urine was collected and
sent for cytologic examination. Microscopic examination of the slide revealed benign
urothelial and squamous cells in a background of acute inflammation and red blood cells.
Incidentally, scattered, small, oval-shaped "cells" with eccentric dark nuclei and gray
cytoplasm with rare red cytoplasmic granules were also seen as indicated in the figure
below. The cytologic findings were consistent with Trichomonas organisms. [Print in
colour]
Page 2 of 6
|
|
3 Page 3 |
▲back to top |
a) What is Trichomoniasis and how is it transmitted?
(4)
b) Describe the cytological features of trichomonas vaginalis.
(6)
c) Differentiate between the two main types of herpes simplex virus.
(4)
Question 3
[17]
3.1 A 61-year-old Malay male who was first diagnosed with hepatocellular carcinoma
presented with progressive jaundice, fever, and abdominal pain for 5 months duration.
There was associated loss of weight of 6 kg. His computed tomography (CT) abdomen
showed evidence of liver cirrhosis. The cause of liver cirrhosis is unknown.
a) Suggest further biochemical tests that can be performed on this patient.
(10)
b) Which haematological tests would you perform for this patient AND what would you
expect your results to be? Motivate your answer.
(4)
C) Briefly describe the histopathological examination that may be performed and its
significance.
(3)
QUESTION 4
[30]
4.1 A 15-year-old Caucasian school girl presented to the Emergency Department {ED)
complaining of a single day history of lower abdominal pain, muscle aches, diarrhoea, and
vomiting. She had a tampon in situ for 24 hours for menstrual bleeding. She had been
undergoing treatment for thyroid nodular disease using carbimazole 10 mg twice daily,
which she had ceased 3 days previously. On initial examination, the patient was
Page 3 of 6
|
|
4 Page 4 |
▲back to top |
hypotensive (systolic blood pressure 75 mmHg), pyrexic (temperature 39.4°(), and
tachycardic (heart rate 150/minute). There were signs of multiorgan dysfunction as her
skin peripheries were profoundly vasoconstricted and mottled with a significant delay in
capillary refill time (10 seconds) and an elevated serum lactate (13.0 mmol/L). The patient
was acutely confused and intermittently drowsy. There was a generalized lower
abdominal tenderness. Vaginal examination revealed a malodorous tampon, coated in a
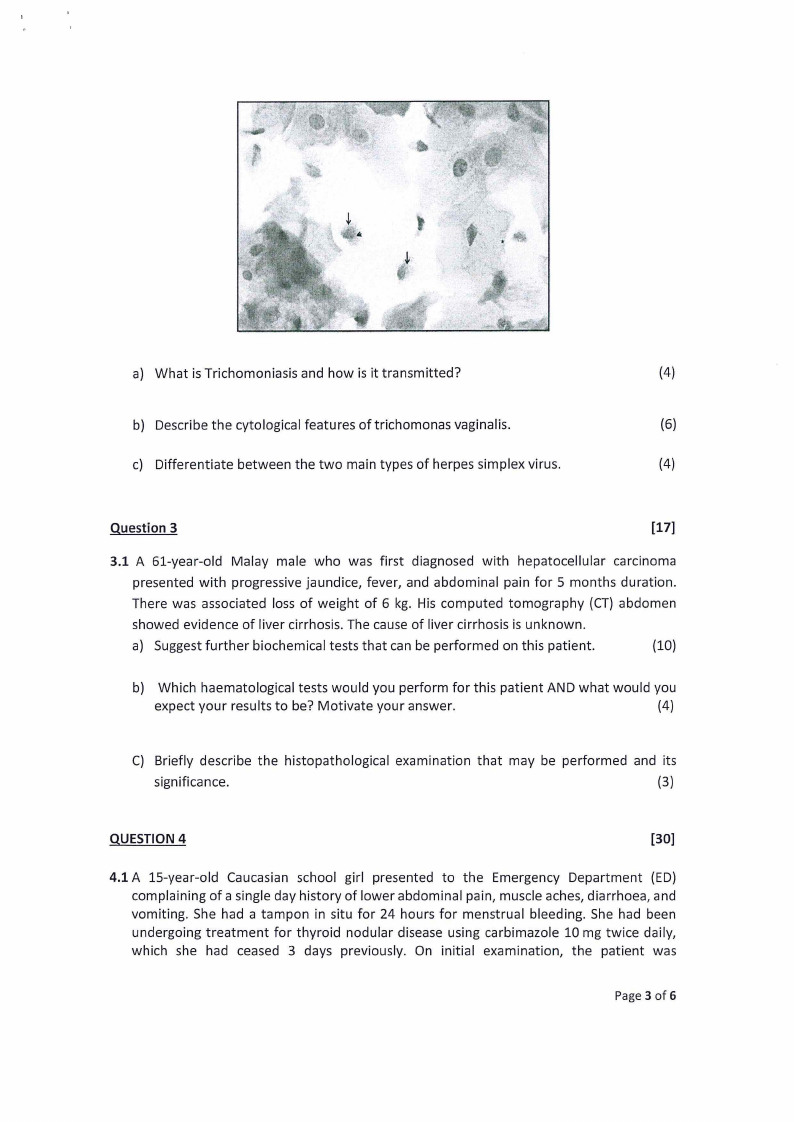
green mucopurulent discharge, which was removed. Laboratory results from a high
vaginal swab from this girl presented with the following:
i) Gram stained slide, ii) Blood agar cultured plate iii) MSA plate
a) What organism is responsible for this infection?
(2)
b) What virulence factors is mostly responsible for the symptoms in this patient?
(2)
c) Suggest the expected abnormalities seen in the full blood count of this patient, and
explain your answer?
(6)
d) Propose the expected CRPresult of this patient and justify your answer.
(20)
QUESTION 5
[8]
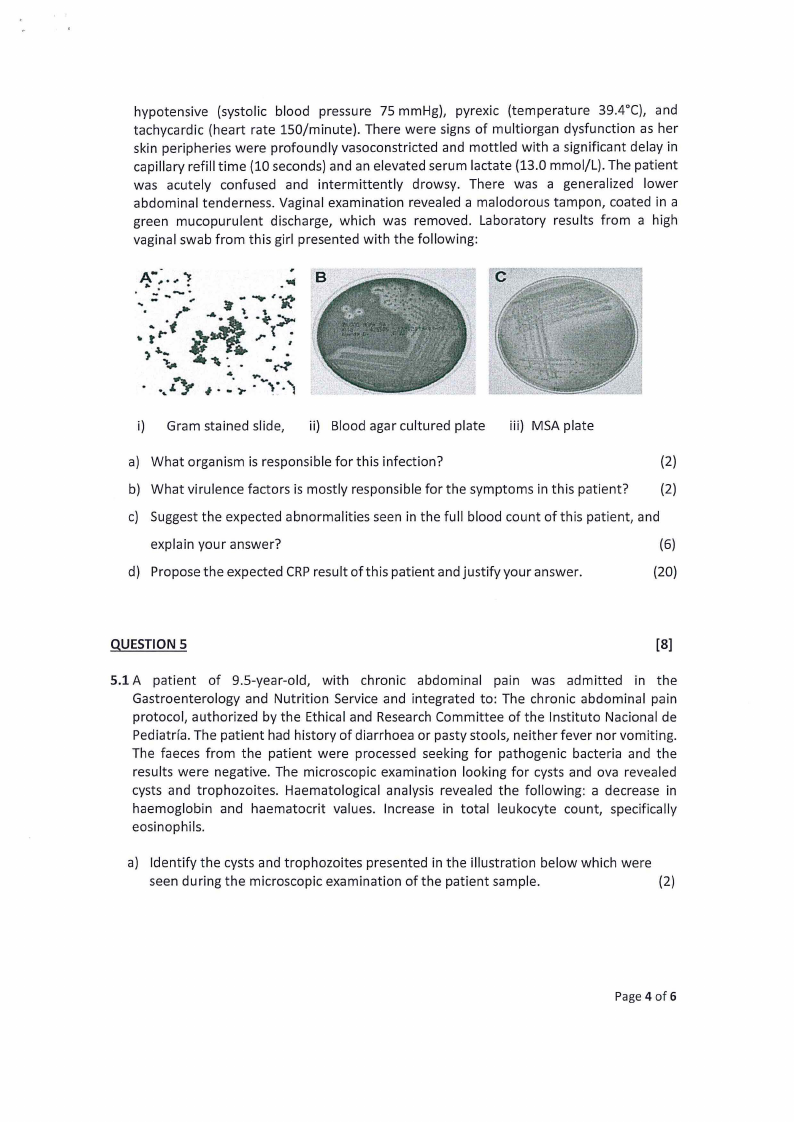
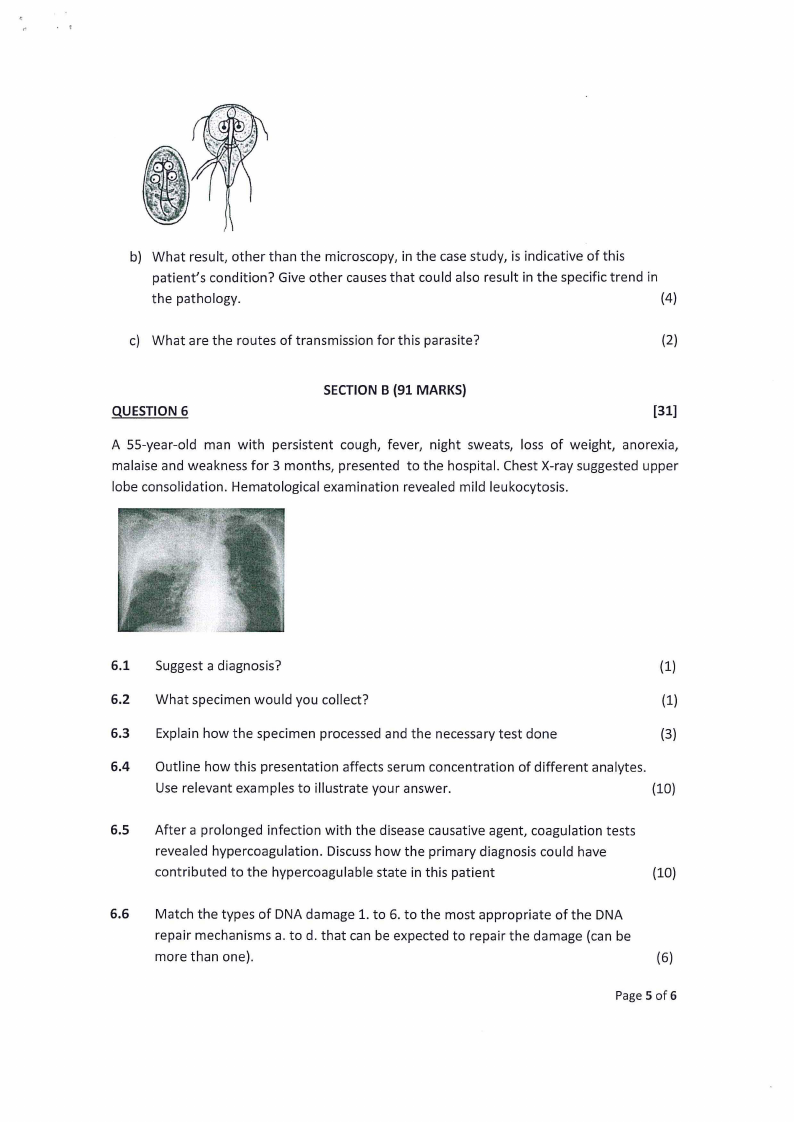
5.1 A patient of 9.5-year-old, with chronic abdominal pain was admitted in the
Gastroenterology and Nutrition Service and integrated to: The chronic abdominal pain
protocol, authorized by the Ethical and Research Committee of the lnstituto Nacional de
Pediatrfa. The patient had history of diarrhoea or pasty stools, neither fever nor vomiting.
The faeces from the patient were processed seeking for pathogenic bacteria and the
results were negative. The microscopic examination looking for cysts and ova revealed
cysts and trophozoites. Haematological analysis revealed the following: a decrease in
haemoglobin and haematocrit values. Increase in total leukocyte count, specifically
eosinophils.
a) Identify the cysts and trophozoites presented in the illustration below which were
seen during the microscopic examination of the patient sample.
(2)
Page 4 of 6
|
|
5 Page 5 |
▲back to top |
.r
b) What result, other than the microscopy, in the case study, is indicative of this
patient's condition? Give other causes that could also result in the specific trend in
the pathology.
(4)
c) What are the routes of transmission for this parasite?
(2)
SECTION B (91 MARKS)
QUESTION 6
[31]
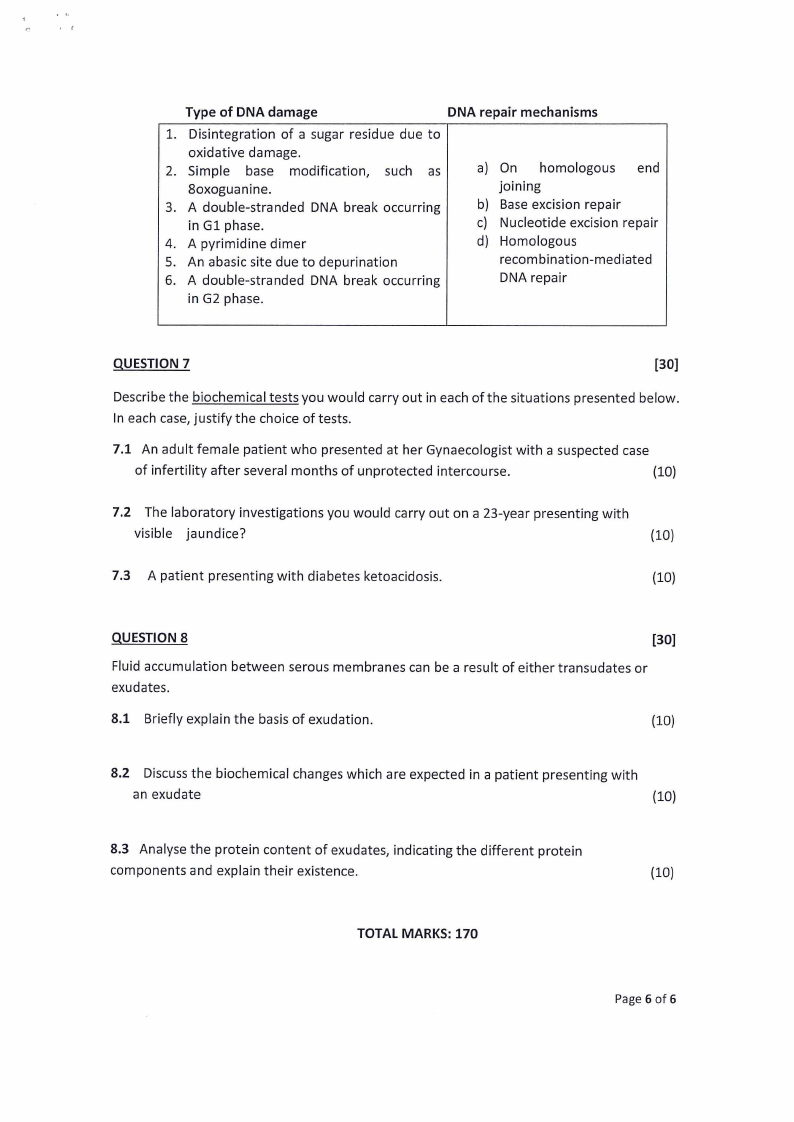
A 55-year-old man with persistent cough, fever, night sweats, loss of weight, anorexia,
malaise and weakness for 3 months, presented to the hospital. Chest X-ray suggested upper
lobe consolidation. Hematological examination revealed mild leukocytosis.
6.1 Suggest a diagnosis?
(1)
6.2 What specimen would you collect?
(1)
6.3 Explain how the specimen processed and the necessary test done
(3)
6.4 Outline how this presentation affects serum concentration of different analytes.
Use relevant examples to illustrate your answer.
{10)
6.5 After a prolonged infection with the disease causative agent, coagulation tests
revealed hypercoagulation. Discuss how the primary diagnosis could have
contributed to the hypercoagulable state in this patient
(10)
6.6 Match the types of DNA damage 1. to 6. to the most appropriate of the DNA
repair mechanisms a. to d. that can be expected to repair the damage (can be
more than one).
(6)
Page 5 of6
|
|
6 Page 6 |
▲back to top |
'(
Type of DNA damage
DNA repair mechanisms
1. Disintegration of a sugar residue due to
oxidative damage.
2. Simple base modification, such as
8oxoguanine.
3. A double-stranded DNA break occurring
in Gl phase.
4. A pyrimidine dimer
5. An abasic site due to depurination
6. A double-stranded DNA break occurring
in G2 phase.
a) On homologous end
joining
b) Base excision repair
c) Nucleotide excision repair
d) Homologous
recombination-mediated
DNA repair
QUESTION 7
[30]
Describe the biochemical tests you would carry out in each of the situations presented below.
In each case, justify the choice of tests.
7.1 An adult female patient who presented at her Gynaecologist with a suspected case
of infertility after several months of unprotected intercourse.
(10)
7.2 The laboratory investigations you would carry out on a 23-year presenting with
visible jaundice?
(10)
7.3 A patient presenting with diabetes ketoacidosis.
(10)
QUESTION 8
[30]
Fluid accumulation between serous membranes can be a result of either transudates or
exudates.
8.1 Briefly explain the basis of exudation.
(10)
8.2 Discuss the biochemical changes which are expected in a patient presenting with
an exudate
(10)
8.3 Analyse the protein content of exudates, indicating the different protein
components and explain their existence.
(10)
TOTAL MARKS: 170
Page 6 of 6