





 |
CLC711S - CLINICAL CHEMISTRY 3- 2ND OPP - JULY 2023 |
|
|
1 Page 1 |
▲back to top |
nAmlBIA unlVERSITY
OF SCIEnCE AnD TECHnOLOGY
FACULTYOF HEALTH,APPLIEDSCIENCESAND NATURALRESOURCES
SCHOOLOF HEALTHSCIENCES
DEPARTMENT OF CLINICALHEALTHSCIENCES
QUALIFICATION:BACHELOROF MEDICAL LABORATORYSCIENCES
QUALIFICATIONCODE: 08BMLS
LEVEL: 7
COURSECODE: CLC711S
COURSENAME: CLINICAL CHEMISTRY 3
SESSION:
JULY 23
PAPER:
THEORY
DURATION: 3 HOURS
MARKS:
100
SECONDOPPORTUNITYEXAMINATION QUESTION PAPER
EXAMINER(S)
MS CARAMIA DUNAISKI
MODERATOR:
DR MUNYARADZI MUKESI
INSTRUCTIONS
1. Answer ALL the questions.
2. Write clearly and neatly.
3. Number the answers clearly.
PERMISSIBLEMATERIALS
1. CALCULATOR
THIS QUESTION PAPERCONSISTSOF 5 PAGES{Including this front page)
|
|
2 Page 2 |
▲back to top |
QUESTION 1
[10]
An 18-year-old woman is referred for investigation of distressing hirsutism. She
shaves daily and has noticed deepening of her voice and scalp hair loss. On
questioning she admits to irregular menstrual periods. On examination she is
clearly hirsute with male-pattern distribution of body hair; temporal balding and
deep voice are confirmed.
Provide a differential diagnosis for androgen excess in an adult female patient and
laboratory/ clinical investigations that will aid in this diagnosis.
QUESTION 2
[15]
Discuss the laboratory investigations necessary to assist in the diagnosis and
management of diseases of the joints.
QUESTION 3
[20]
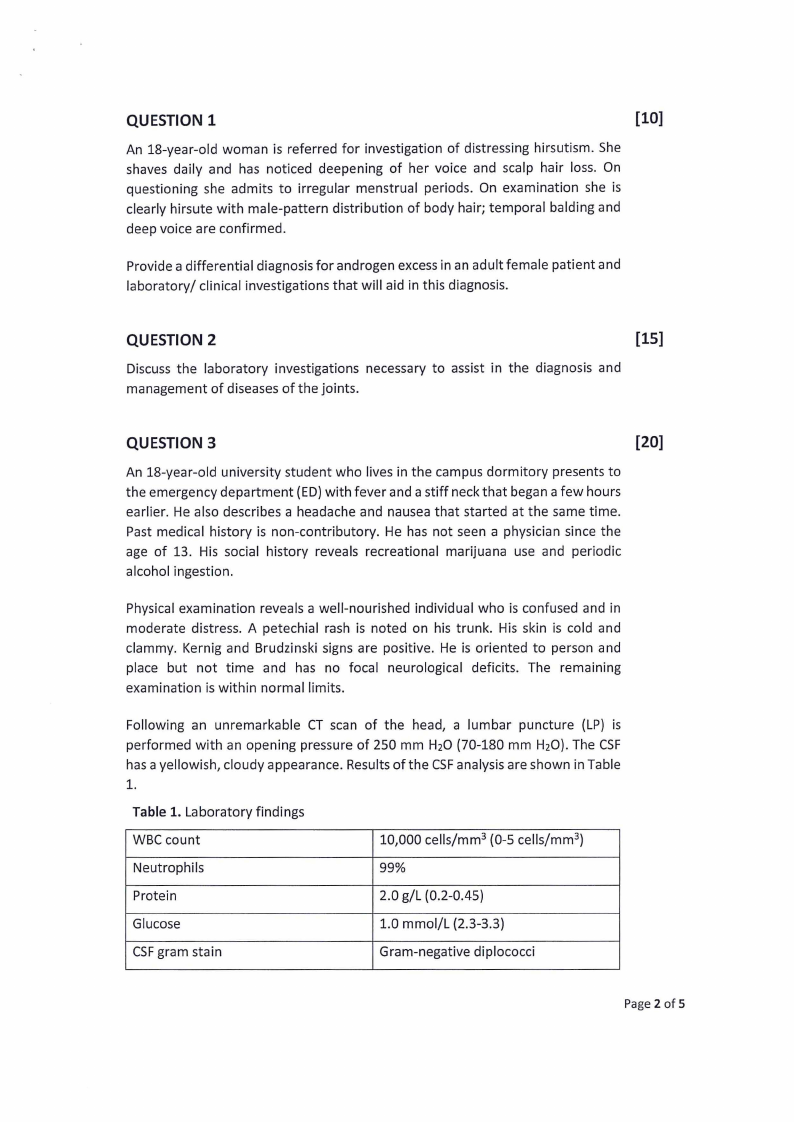
An 18-year-old university student who lives in the campus dormitory presents to
the emergency department (ED) with fever and a stiff neck that began a few hours
earlier. He also describes a headache and nausea that started at the same time.
Past medical history is non-contributory. He has not seen a physician since the
age of 13. His social history reveals recreational marijuana use and periodic
alcohol ingestion.
Physical examination reveals a well-nourished individual who is confused and in
moderate distress. A petechial rash is noted on his trunk. His skin is cold and
clammy. Kernig and Brudzinski signs are positive. He is oriented to person and
place but not time and has no focal neurological deficits. The remaining
examination is within normal limits.
Following an unremarkable CT scan of the head, a lumbar puncture (LP) is
performed with an opening pressure of 250 mm H2O (70-180 mm H2O). The CSF
has a yellowish, cloudy appearance. Results of the CSFanalysis are shown in Table
1.
Table 1. Laboratory findings
WBC count
10,000 cells/mm 3 (0-5 cells/mm 3)
Neutrophils
99%
Protein
2.0 g/L (0.2-0.45)
Glucose
1.0 mmol/L (2.3-3.3)
CSFgram stain
Gram-negative diplococci
Page 2 of 5
|
|
3 Page 3 |
▲back to top |
Given the patient's age and laboratory results, provide the most likely diagnosis
and give a detailed description ofthe significance of collecting a CSFsample in this
particular patient, and how it will aid in the diagnosis of disease.
Three marks will be allocated to the most likely diagnosis, ten marks will be
allocated to CSFdescription and specimen significance and seven marks will be
allocated to importance in CSFanalysis in the diagnosis of disease.
QUESTION 4
[20]
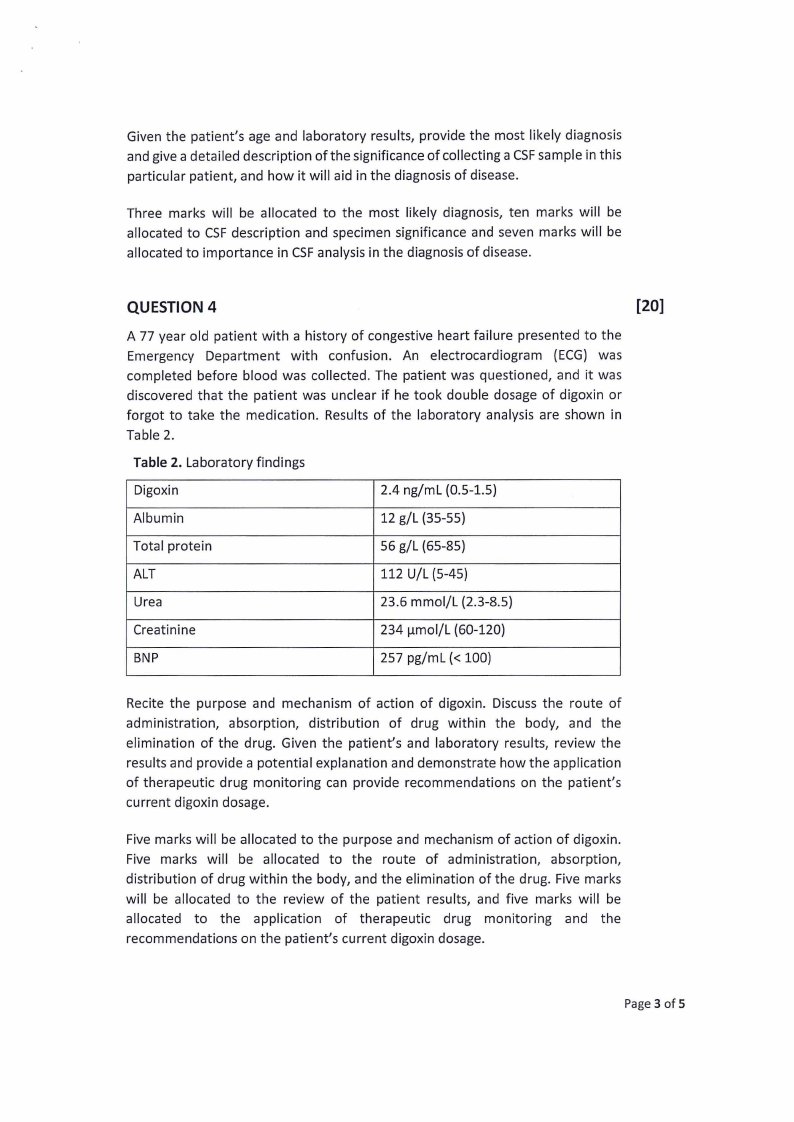
A 77 year old patient with a history of congestive heart failure presented to the
Emergency Department with confusion. An electrocardiogram {ECG) was
completed before blood was collected. The patient was questioned, and it was
discovered that the patient was unclear if he took double dosage of digoxin or
forgot to take the medication. Results of the laboratory analysis are shown in
Table 2.
Table 2. Laboratory findings
Digoxin
2.4 ng/ml (0.5-1.5)
Albumin
12 g/L {35-55)
Total protein
56 g/L {65-85)
ALT
112 U/L (5-45)
Urea
23.6 mmol/L (2.3-8.5)
Creatinine
234 µmol/L (60-120)
BNP
257 pg/ml(< 100)
Recite the purpose and mechanism of action of digoxin. Discuss the route of
administration, absorption, distribution of drug within the body, and the
elimination of the drug. Given the patient's and laboratory results, review the
results and provide a potential explanation and demonstrate how the application
of therapeutic drug monitoring can provide recommendations on the patient's
current digoxin dosage.
Five marks will be allocated to the purpose and mechanism of action of digoxin.
Five marks will be allocated to the route of administration, absorption,
distribution of drug within the body, and the elimination of the drug. Five marks
will be allocated to the review of the patient results, and five marks will be
allocated to the application of therapeutic drug monitoring and the
recommendations on the patient's current digoxin dosage.
Page 3 of 5
|
|
4 Page 4 |
▲back to top |
QUESTION 5
[15]
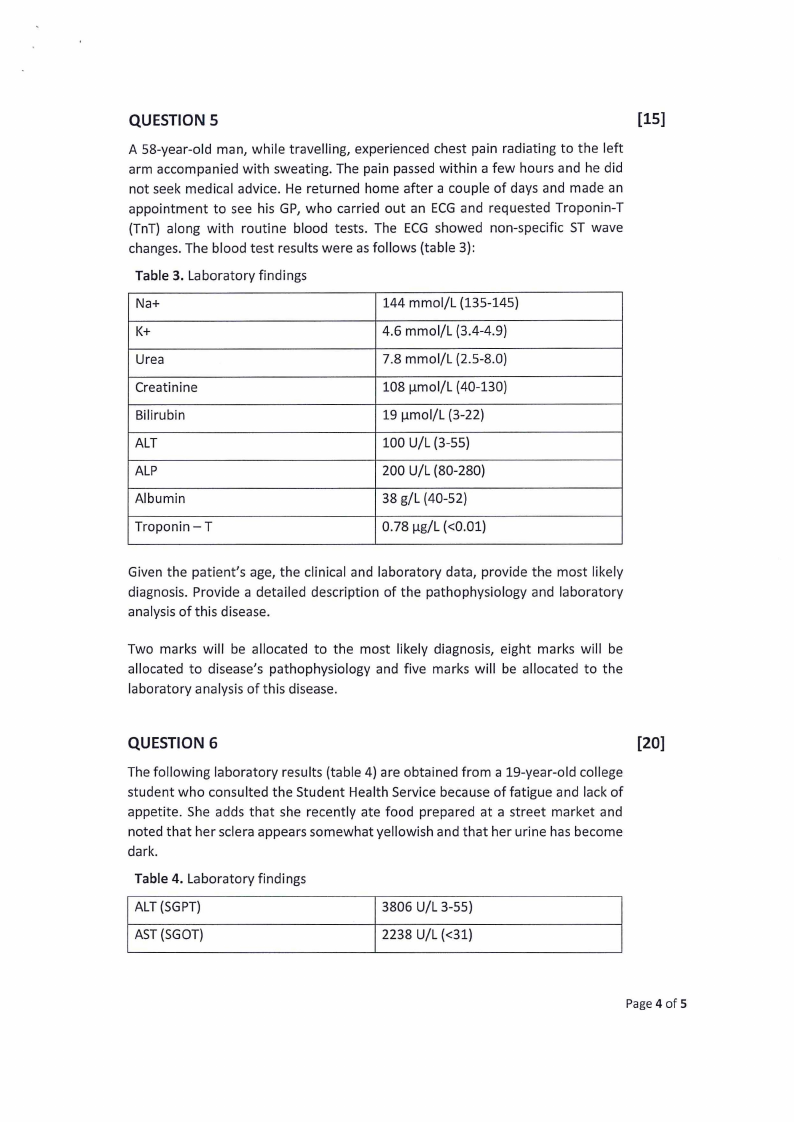
A 58-year-old man, while travelling, experienced chest pain radiating to the left
arm accompanied with sweating. The pain passed within a few hours and he did
not seek medical advice. He returned home after a couple of days and made an
appointment to see his GP, who carried out an ECGand requested Troponin-T
(TnT} along with routine blood tests. The ECG showed non-specific ST wave
changes. The blood test results were as follows (table 3}:
Table 3. Laboratory findings
Na+
144 mmol/L (135-145}
K+
4.6 mmol/L (3.4-4.9}
Urea
7.8 mmol/L (2.5-8.0}
Creatinine
108 µmol/L (40-130}
Bilirubin
19 µmol/L (3-22}
ALT
100 U/L (3-55}
ALP
200 U/L (80-280}
Albumin
38 g/L (40-52}
Troponin-T
0.78 µg/L (<0.01}
Given the patient's age, the clinical and laboratory data, provide the most likely
diagnosis. Provide a detailed description of the pathophysiology and laboratory
analysis of this disease.
Two marks will be allocated to the most likely diagnosis, eight marks will be
allocated to disease's pathophysiology and five marks will be allocated to the
laboratory analysis of this disease.
QUESTION 6
[20]
The following laboratory results (table 4} are obtained from a 19-year-old college
student who consulted the Student Health Service because of fatigue and lack of
appetite. She adds that she recently ate food prepared at a street market and
noted that her sclera appears somewhat yellowish and that her urine has become
dark.
Table 4. Laboratory findings
ALT (SGPT}
3806 U/L 3-55}
AST (SGOT}
2238 U/L (<31}
Page 4 of 5
|
|
5 Page 5 |
▲back to top |
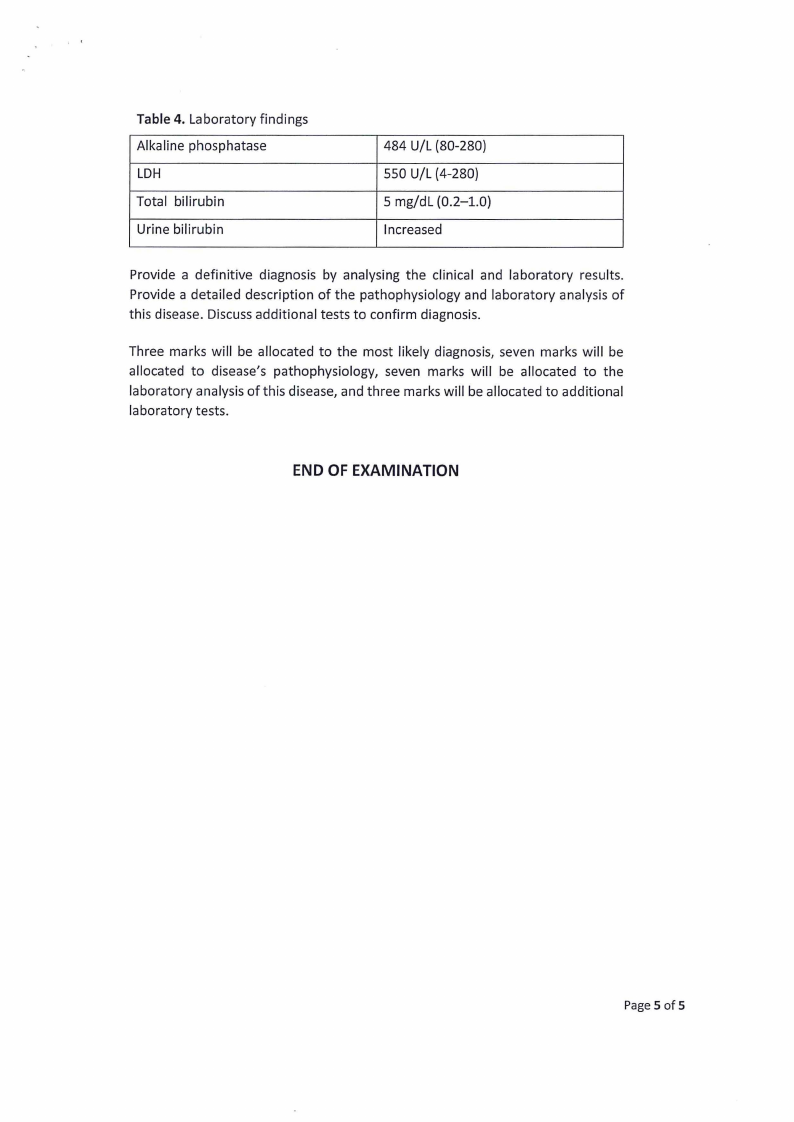
Table 4. Laboratory findings
Alkaline phosphatase
LDH
Total bilirubin
Urine bilirubin
484 U/L (80-280}
550 U/L (4-280}
5 mg/dl (0.2-1.0}
Increased
Provide a definitive diagnosis by analysing the clinical and laboratory results.
Provide a detailed description of the pathophysiology and laboratory analysis of
this disease. Discuss additional tests to confirm diagnosis.
Three marks will be allocated to the most likely diagnosis, seven marks will be
allocated to disease's pathophysiology, seven marks will be allocated to the
laboratory analysis of this disease, and three marks will be allocated to additional
laboratory tests.
END OF EXAMINATION
Page 5 of 5